

You are leaving this site!
By clicking YES, you will be directed to another website. Click NO to remain on this page. Do you wish to continue to another website?
Intended for U.S. audiences only
Intended for U.S. audiences only


Once someone is exposed to HBV and remains unprotected, HBV may
take hold and develop into potentially deadly chronic liver disease7
HBV=hepatitis B virus; HIV=human immunodeficiency virus; STIs=sexually transmitted infections.
What immediate steps will you take to help protect your
patients from developing a chronic HBV infection?


Anti-HBs=anti-hepatitis B surface antibodies; IU=international units; WHO=World Health Organization.
CDC Recommendations for Prophylaxis:
Administering an HBIG with the HBV vaccine series is highly effective in
preventing transmission following exposure to HBV14
Patients with mild reactions related to the administration of Nabi-HB (N=50)12
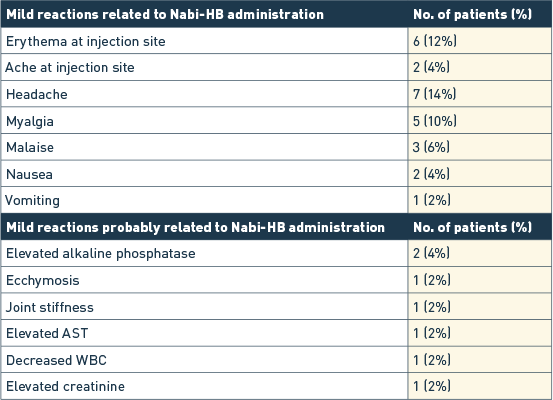
AST=aspartate transaminase; WBC=white blood cells.
Nabi-HB is a market leader with a proven safety profile12,13
References:
Individuals known to have had an anaphylactic or severe systemic reaction to human globulin should not receive Nabi-HB® [Hepatitis B Immune Globulin (Human)] or any other human immune globulin. Individuals who are deficient in IgA have the potential to develop antibodies against IgA and anaphylactic reactions.
In patients who have severe thrombocytopenia or any coagulation disorder that would contraindicate intramuscular injections, Nabi-HB should be given only if the expected benefits outweigh the potential risks.
Nabi-HB is made from human plasma. Products made from human plasma may carry a risk of transmitting infectious agents (e.g., viruses) and, theoretically, the Creutzfeldt-Jakob disease (CJD) agent.
Nabi-HB [Hepatitis B Immune Globulin (Human)], must be administered only intramuscularly for post-exposure prophylaxis.
Vaccination with live virus vaccines (e.g., MMR) should be deferred until approximately three months after administration of Nabi-HB.
The most common adverse reactions associated with Nabi-HB in clinical trials were erythema and ache at the injection site as well as systemic reactions such as headache, myalgia, malaise, nausea and vomiting. No anaphylactic reactions with Nabi-HB have been reported.
Please see the full Prescribing Information for Nabi-HB [Hepatitis B Immune Globulin (Human)].
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/MedWatch or call 1-800-FDA-1088.